




Miranda Moore
RDA Lead Assistant, Beacon Dentistry
Your go-to source for insights, tips, and real stories from the front lines of dental practice management. Whether you're looking to cut costs, streamline your workflow, or stay ahead of industry trends—we’re here to help. We share what we’ve learned working with hundreds of practices across the country, so you can focus on what matters most: delivering great care.
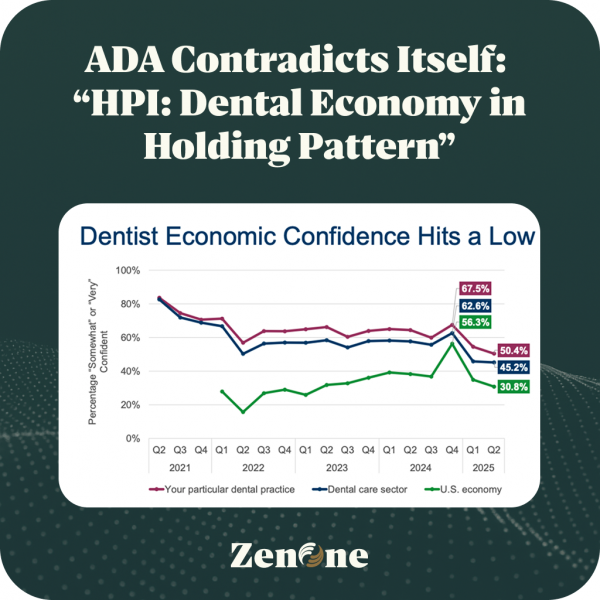
My take on the Q2 2025 ADA HPI ReportFull report link What is the ADA doing here? Yes, dentists are

As we collectively let out a sigh of relief that the COVID-19 pandemic is nearing it’s end in May, it

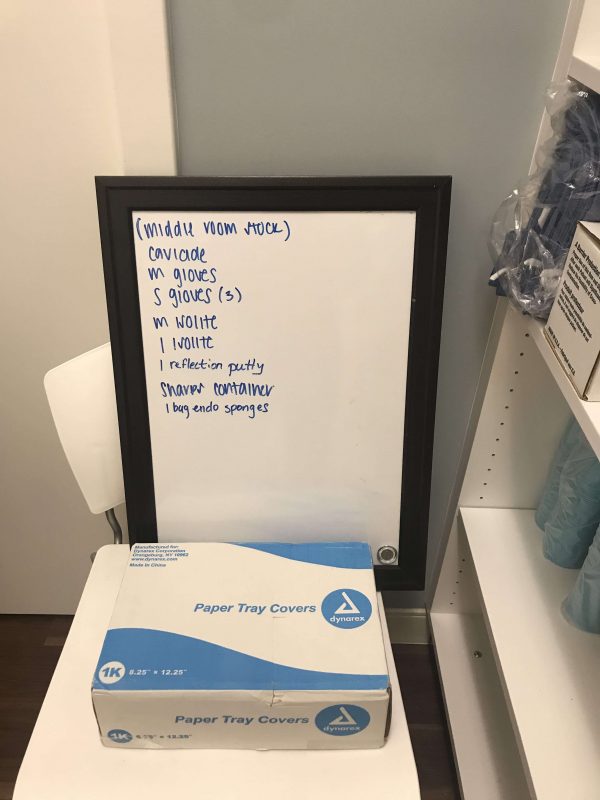
10 Things Every Assistant Should know about Infection Control: PPEs – 4 items – mask; gloves; goggles; gown Utility Gloves

This is a repost from Becker’s Healthcare, written by Gabrielle Masson on March 30, 2020. President Donald Trump passed a

The Centers for Disease Control and Prevention (CDC) set the water quality standard for dental unit treatment water at ≤500CFU/ml
Dental practices have faced numerous challenges this year, due to the COVID-19 pandemic and those challenges continue. As the
Continue reading
Customer Stories
Dr. Jack Fan
Practice Owner, The Dental Centre
“Now we’re no longer tied to one distributor — if something’s out of stock, we just find it elsewhere. My assistants handle everything, and it’s one less thing on my plate.”
Read More
Dr. Benjamin A Johnson
Practice Owner, Acre Wood Dental - Waco
“We stay on budget, we have the supplies when we need them, and my input is almost zero — exactly how a business should run.”
Read More
Dr. Justin Louie
Practice Owner, Advanced Dental Care of Austin
"Now we get quality materials for less by comparing products and suppliers directly in ZenOne."
Read More
Message Successfully Sent!
Thanks for getting in touch! A member of our team will respond to your message within the next 48 hours.
Ok
Start Your Free Trial
Every ZenOne trial begins with our most powerful plan, so you can explore all the features and savings without limits. After your trial, you can choose to stay at the full level or request to downgrade— whatever fits your practice best.
By joining Zen, you’re not just signing up for software—you’re joining a movement that empowers private practices to stay private. Every practice that joins adds to the collective volume we use to negotiate even better pricing for everyone.

